
New examination and treatment method (NUB)
New examination and treatment method (NUB)
Summary
In this overview, you will learn everything you need to know about the procedure for New Examination and Treatment Methods (Neue Untersuchungs- und Behandlungsmethoden, NUB) as a manufacturer of an innovative technology. Furthermore, you will find out how you can use this Fast Track process to obtain specific reimbursement for your product. Initially, it is not relevant whether the treatment method is a medical device or a drug.
You will learn how you can find out whether your treatment method is eligible for NUB and what the different NUB procedures are. You will understand if and how these procedures are related to each other, how they are structured, which one is relevant for you and where you should take advantage of opportunities and avoid dangers.
We will inform you why the NUB process exists and what the essential points of the process are. Furthermore, you will learn how to prepare for the NUB process to avoid mistakes and unnecessary risks.
What is the NUB-procedure (definition)?
There are two different NUB procedures. They are regulated by different laws with different goals and have very little in common.
The NUB procedure is an application procedure through which hospitals can obtain the opportunity to negotiate extrabudgetary reimbursement with payers.
The NUB procedure to which we refer here is the procedure according to section 6 para. 2 KHEntgG (Hospital Remuneration Act). It was implemented together with the DRG-system. However, it differs significantly from the DRG procedure according to § 137h SGB V. Subsequently, we will refer to the procedure according to section 6 para. 2 KHEntgG as the "NUB procedure".
Why is there a NUB-procedure?
The NUB procedure is intended to close the so-called calculation gap in the G-DRG system. The calculation gap is a period of about two to three years. This is the minimum time it takes for the costs of innovative technologies to be included in the G-DRG system. The calculation gap can also last longer.
Background information:
A All in-patient services provided in German hospitals are reimbursed via the G-DRG system. The service identifiers (e.g., OPS-codes, ICD-10-GM-codes, age, gender, weight, date of surgery, etc.) are used to assign a single DRG to each individual treatment case. This DRG is assigned a valuation ratio (relative weight) which, when multiplied by a base case value, yields the final DRG reimbursement.
The relative weight is calculated annually by the InEK. In the process, cases are grouped into case groups (DRGs) according to their costs and on the basis of their medical service designators. The average costs of the cases in such a group are divided by the so-called reference value, resulting in the non-dimensional relative weight.
This means that the reimbursement via the DRG system is dependent on the costs of the treatment cases of the previous years. The InEK calculates the average costs and thus also the reimbursement of the DRGs one year before they are valid on the basis of service and cost data incurred in the preceding year. This results in a delay of 2 years. Specific OPS-codes are typically required to identify the cases, which must first be applied for and then be established, which takes at least another year.
The NUB process is intended to close this time gap - the calculation gap.
Who can submit a NUB-proposal?
In principle, a NUB application can be submitted by all German hospitals.
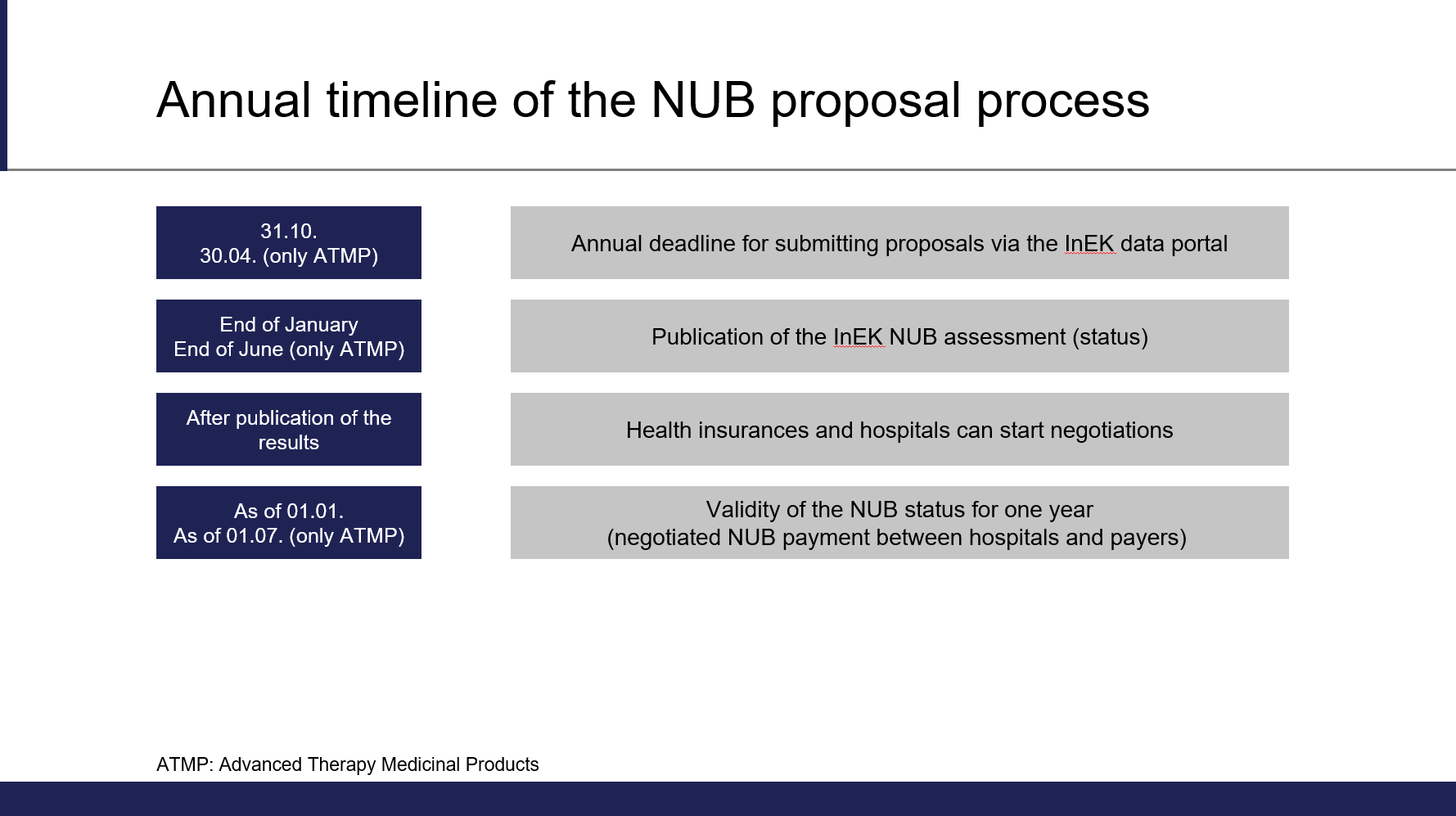
Hospitals will be able to agree on individual reimbursement for innovative technologies with the health insurances. A requirement is that the technologies are not yet appropriately reimbursed under the DRG lump sum system and each hospital must submit a NUB proposal individually. Proposal must be submitted to the German Institut for Reimbursement in Hospitals (Institut für das Entgeltsystem im Krankenhaus, InEK) by October 31st of each year.

Carefully conduct a market analysis on the German healthcare market and evaluate which hospitals are suitable to use your technology in the following year. Only hospitals that submitted an application in time are generally considered for NUB payment.

Who decides on NUB-proposals?
The InEK decides on all NUB applications as a whole. All NUB proposals are combined into a single topic and the information is evaluated overall. The aim is to ensure that all proposals for a NUB procedure are given the same status.
The InEK evaluates the NUB proposals without further data. A proposal with poor content can jeopardize the evaluation of a entire treatment. Do not give away the preparation of a proposal, we will show you how it is supposed to be done.
Who compiles the NUB-proposals?
This varies widely. In many cases, NUB proposals are prepared, written and submitted by physicians or even by medical controllers in hospitals. NUB proposals are primarily economical and not medical proposals. Based on our experience, collaboration with clinically active physicians is absolutely necessary when preparing a proposal, and they should be prepared with specialized consultants. In addition, NUB proposals submitted to the InEK by different hospitals on the same topic are reviewed as one. Therefore, it has proven to be useful for specialized consultants to prepare one NUB proposals for the respective therapies on behalf of the industry.
Take advantage of your opportunities in the NUB process and get support from specialized experts.
How can you distribute NUB proposals to various hospitals?
There are different methods to distribute NUB proposals to hospitals. There is the NUB exchange or websites of professional societies where one can download the respective NUB proposals. We prefer a different method, which has shown to be particularly successful.
Keep control of applications and their distribution. Organize the distribution of NUB proposals as well-thought-out NUB proposal management. We will tell you how!
How does the NUB procedure work?
Once a NUB proposal has been prepared and sent to the hospital, the hospital must submit it to the InEK via the InEK data portal by October 31st.
At the InEK, all proposals are then reviewed, summarized by topic, and evaluated based on the information in the proposals. Typically, the evaluation of the proposals takes place by the end of January of the following year and are published subsequently.
Is Reimbursement guaranteed if a therapy has been assigned NUB status 1?
NUB status 1 means, among other things, that the method is so new that it cannot yet be represented appropriately by a lump sum per case due to the calculation procedure.
With this information, the applying hospitals can then agree on an individual charge for the service with the health insurances or their negotiating partners (as a difference to the respective G-DRG).
Support your customers, the hospitals, in their preparation for negotiations with the payers. Over the past few years, Healthcare Heads has developed a comprehensive service package with which hospitals can be comprehensively supported in the context of a NUB proposal.
How is an individual Reimbursement agreed upon?
The operating costs of hospital treatments are financed by the health insurances through the DRG-system. The hospital budget (care budget) for a year is negotiated by the hospitals and the health insurances. This typically happens once a year. In many cases, NUB charges are also discussed as part of this budget negotiation, although NUB charges are also valid without this negotiation.
Depending on the service, hospitals must demonstrate to the health insurances that the service is to be reimbursed in accordance with the rules of SGB V.
The next step is to determine the amount of compensation on an individual basis, which can be difficult. The hospital has to calculate the differential costs of the method - similar to the NUB proposal itself - in relation to the G-DRG. In doing so, the typical costs of treatment cases in the respective per-case flat rate must be deducted from the relevant costs caused by the innovative therapy.
These data form the basis for negotiating the number and amount of the corresponding NUB payments with the payers.
A NUB proposal - even if it has received status 1 from the InEK - only becomes successful through negotiations with the health insurances. It is useful to support your customers to become successful with your treatment method.
Which NUB statuses are there and what do they mean?
NUB-status 1 (or 11)
With NUB status 1, you have reached your destination. The method is considered new and not appropriately represented in the DRG-system and can be negotiated with the health insurances.
NUB-status 2
If a method was assessed by the InEK with NUB status 2, the NUB proposal does not meet the required criteria. Negotiation of a NUB payment in accordance with sec. 6 para. 2 KHEntgG between the requesting hospital and the health insurance is therefore not allowed. There are various reasons that can lead to a status 2, including poorly prepared, incomplete or incorrectly completed proposals or poor NUB management. This means that it may make sense to revise a NUB proposal and re-submit it the following year.
Being assigned NUB status 2 may be due to the treatment method or the proposal itself. In principle, it is possible to convert a proposal with a NUB status 2 to a NUB status 1 in the following year. Take advantage of our consultation as part of the NUB 2nd look process.
NUB status 3
If a method is given NUB status 3, it means that the InEK was not able to fully process the proposals within the deadline to make a final assessment. To our knowledge, this situation has so far only occurred in the year of the introduction of the NUB process.
NUB-status 4 (or. 41)
If a method received NUB status 4 from the InEK, the information contained in the proposal is implausible or cannot be reconstructed. Thus, the InEK does not have sufficient information on the method according to sec. 6 para. 2 KHEntgG. In exceptional cases, a NUB payment may nevertheless be negotiated between the hospital and the health insurance for services that have been evaluated with status 4.
Since 2021, there are also special statuses with separate deadlines for ATMP therapies (drugs for new therapies within the meaning of sec. 4 para. 9 of the German Medicines Act). This concerns, for example, CAR-T-Cell therapy. These therapies will not be discussed further in this article. If you are interested in participating in the NUB procedure with a corresponding drug, there are specifics to be considered, which we will be happy to explain to you in a personal conversation.

When is the deadline for NUB submissions?
The term NUB refers to "new examination and treatment methods". The term "new" plays an important role here. If a proposal is submitted too late, the procedure may no longer be "new" within the meaning of sec. 6 para. 2 KHEntgG.
Do you already have approval for your innovative procedure (CE marking according to MDD or MDR) and are you planning to offer your service in German hospitals? Then you should consider a NUB proposal, in particular if your innovative technology is associated with high, DRG-relevant costs that are not yet represented in the DRG-system. The NUB proposal for the following year must be submitted by October 31st. Proposals must be submitted by the hospitals providing the service and wishing to negotiate payment for it with the health insurances.
It is rare to be too early with a proposal, being too late is much more likely. Are you wondering if you already have all necessary evidence, data and documents? Make a non-binding appointment with us, we can help you shortly.
How is a NUB proposal submitted?
There is a special application form for the NUB procedure, which must be completed online at the InEK’s website. Each hospital must complete this form and submit it to the InEK via the data portal by the deadline of October 31st.
Important!
The proposal consists of a large number of specific questions, the content of which must always be completed in the context of the G-DRG system and sec. 6 para. 2 KHEntgG.
The NUB procedure takes place at the InEK. The institute makes reimbursement decisions without a data basis, which is why the data basis must be plausibly presented to the InEK in the NUB proposal.
Use experts who specialize in NUB proposals and who have extensive experience to help you complete the proposal.
What role does the industry play in the NUB application?
A distinction must be made between the NUB procedure pursuant to sec. 6 para. 2 KHEntgG and the procedure according to sec. 137h SGB V.
The industry does not have an official role in the NUB procedure. However, sec. 137h SGB V requires that a NUB proposal must be submitted by hospitals in agreement with the manufacturer of the medical device.
The industry therefore has a legally induced interest as well as an interest in prompt and appropriate reimbursement by the health insurance funds for products that in many cases are the prerequisite for innovative therapies.
It has proven helpful and has therefore become established in Germany that the manufacturers commission experts to fill out the NUB proposals correctly and professionally and to organize the NUB procedure for them.
You only have a few attempts to get everything right in the NUB process. Get advice and support from a NUB expert right from the start to guide you through all process steps on the way to regulated and appropriate reimbursement.
What requirements must be met for an innovation to receive status 1?
The NUB procedure according to sec. 6 para. 2 KHEntgG serves to close the so-called OPS calculation gap. Accordingly, a service must have high DRG-relevant costs that are not yet properly represented in the DRG-system due to the market launch and the time lapse of the calculation gap. This connection must be explained in a NUB proposal with reference to relevant and additional costs as well as savings compared to the relevant comparative therapies.
You will need very in-depth knowledge of the way the DRG-system works in order to present the economic benefits clearly according to the InEK's ideas. Get support on this topic from experienced experts.
Which accompanying conditions must be met to support a NUB proposal?
In general, "only" the correct, complete and timely submission of a NUB proposal is required from an eligible hospital.
However, experience has shown that, depending on the therapy, various accompanying and general conditions can apply as prequalifying factors for a proposal. What these are always depends on the service, the costs, the potential service providers, the market volume and other parameters.
Start planning the NUB proposal process well in advance. Typically, managing the framework takes longer than completing, writing, and submitting a NUB proposal itself, but proper management can have a lasting impact on the success of a NUB proposal.
When is a therapy new?
Whether a therapy is new within the meaning of the NUB procedure (following sec. 6 para. 2 KHEntgG) does not depend on whether it is a new scientific or new theoretical procedure (sec. 137h SGB V). It only depends on when the procedure was introduced in Germany, in which hospitals and what volume was introduced, and what role these data play in closing the calculation gap.
Do not confuse the term "new" in sec. 6 para. 2 KHEntgG with the term "new" according to sec. 137h SGB V.
When is a therapy reimbursed appropriately?
There is no fixed amount that is determined as appropriately. Whether a therapy is adequately reimbursed depends on the material costs, the personnel costs, which are ultimately also determined by the length of stay, the length of stay, etc., and must be reassessed for each therapy, implant and medical device in relation to the DRG. There may also be other factors that play a role in the consideration of suitable reimbursement.
You can reuse the information and economic model you develop and use as basis for the NUB proposal to support calculation hospitals in the NUB payment negotiations.
Does the NUB procedure also apply to drugs?
In principle, the NUB procedure applies to all services with DRG-relevant costs (individual and actual cost consumption per patient during an in-patient stay). This means that NUB reimbursement is possible for medical devices, drugs, cell therapies and biological procedures as well as for diagnostic methods.
Does the NUB procedure only apply to single-use items?
It is important that the costs are high and DRG-relevant. Investment costs are not reimbursed through the DRG-system under dual financing, for example, but are carried by the German Federal States (Länder). Accordingly, investment costs (or costs of bedside care) fall outside the definition for a NUB payment calculation and are not to be regarded here.
The cost-accounting differentiation from non-DRG-relevant costs as well as the allocation of DRG-relevant costs within the framework of an economic model and the correct naming and plausible description within a NUB proposal are all important aspects.

What are the advantages of clinical studies and clinical evidence for a NUB proposal?
Generally, it should be noted that the NUB procedure according to sec. 6 para. 2 KHEntgG is not a process in which clinical evidence is evaluated. It is judged whether DRG-relevant costs are present in a particular amount and whether the innovation is so new that the costs have not yet arrived or been priced into the DRG-system. Of course, it is helpful to communicate the medical need and benefit, but clinical evidence is not a prerequisite to obtain NUB status 1. On the contrary, the more clinical evidence there is, the older the therapies typically are and tend not to fulfill the criteria of being new.
Think carefully and discuss with your advisor whether it makes sense to submit information on clinical evidence (publications, studies, meta-analyses) and how you can use this to support the proposal.
It is our understanding that a carefully and completely filled out NUB proposal contains everything needed to achieve NUB status 1. It also contains economic information. We do not believe that the submission of additional data is necessary.
Economic data and the right perspective play a crucial role in the evaluation of a NUB proposal. Health economic calculations, budget impact or other modelling, on the other hand, hardly have a positive influence on the NUB evaluation.
What data is the NUB procedure based on?
The NUB procedure is the only process in the InEK that does not require a review of reliable data. This makes it all the more important to present the various facts and the context in the NUB proposal. Of course, this data must reflect the accurate situation, because all information that can be verified is checked in order to assess the reliability and plausibility of the proposal.
A plausible compilation of all the information needed to make a decision as to whether the service is "new" and "not appropriately" represented in the DRG-system in the proposal is important. Please seek advice from experienced experts in this regard.
What can I do if a NUB proposal has already been assigned status 2?
There are many reasons why a NUB proposal is assigned status 2. The typical reasons are that the method is not new within the meaning of the NUB procedure according to sec. 6 para. 2 KHEntgG or that the method is already appropriately represented in the DRG-system.
A method is given NUB status of 2 if only one of these two criteria is met or is not plausibly described in the NUB proposal and leaves doubt whether the procedure is new and not represented appropriately. "Poorly" written proposals, missing information or inconsistent information in several proposals on the same topic can also produce this result. In such cases, a different result can be achieved by making changes in the NUB proposal. For a layperson, it is often difficult to assess whether the method itself is not appropriate for a NUB or whether the information in the proposal has led to this assessment.
We have developed a so-called "NUB 2nd Look" for these cases. Under certain circumstances, services that have been used on the German market for longer than two years can also be assessed with a NUB status 1. Let a versed expert advise you on this matter. We will check for you whether a revision of a NUB proposal makes sense.
The further development of the DRG-system is a possibility to gain reimbursement for services that are not appropriately represented in the system, regardless of whether they are new or not. This proposal procedure is a structured dialog for the involvement of scientific and other expertise in the further development of the G-DRG-system.
If a NUB proposal has received status 2, one solution may be to achieve better reimbursement through the DRG proposal procedure. The DRG proposal procedure is a regulated process open to the industry with an application deadline at the end of February (or March).
Contact us if you are unsure which reimbursement pathway is best for your technology.
Are there other NUB procedures besides the one in sec. 6 para. 2 KHEntgG?
Sec. 137h of the German Social Code, Book V also includes an evaluation of new examination and treatment methods. This evaluation is carried out by the Federal Joint Committee (G-BA) only for medical devices of high-risk classes (IIb and III).
This procedure is only applicable if an inquiry is made to the InEK for the first time in accordance with sec. 6 para. 2 cl. 3 of the KHEntgG. Then, the hospital must provide the G-BA with the state of scientific knowledge of this method as well as with the application in the form of clinical studies with the medical device (only for devices of high-risk classes) in agreement with the manufacturer. Only if the method shows a new theoretical-scientific concept will an evaluation be carried out. This evaluation does not influence the decision of the InEK.
Check very well whether you have a chance of receiving NUB status 1 for methods of high-risk classes and to what extent consultation and information by the G-BA according to sec. 137h SGB V is necessary.
Are there risks in participating in a NUB procedure?
The risk depends on whether your technology is a medical device with a particularly invasive character or classified in the high-risk class IIb or III, whether it is based on a new theoretical-scientific concept, and whether it is the first time a NUB proposal is submitted according to section 6 para. 2 KHEntgG.
For all other technologies, there is basically no risk if a NUB proposal is submitted to the InEK.
However, if no NUB proposal is submitted, there is the risk of not achieving a status 1 rating for the new technology.
Innovative technologies that are based on a new theoretical-scientific concept or are particularly invasive belong to the medical device classes IIb or III. A separate assessment of risk is necessary for products that have never been the subject of a NUB proposal to the InEK in accordance with sec. 6 para. 2 (KHEntgG).
What do the two NUB procedures have to do with each other?
The NUB procedure according to sec. 6 para. 2 KHEntgG and the NUB procedure under sec. 137h SGB V have two different objectives.
A NUB proposal according to sec. 6 para. 2 KHEntgG can trigger a NUB procedure at the German General Joint Committee (Gemeinsamer Bundesausschuss, G-BA) for products of high-risk classes that involve a new theoretical-scientific concept. Conversely, a NUB procedure at the G-BA has no effect on the assessment of a method as a NUB pursuant to sec. 6 para. 2 KHEntgG, unless the method is subsequently excluded from reimbursement.
While the NUB process at the InEK is only about evaluating whether a method is new (time frame) and not appropriately represented in the G-DRG-system, the NUB process at the G-BA is about assessing whether it is a new theoretical-scientific concept and whether the method needs to be excluded from reimbursement due to the evidence.
It is likely that health insurances will require a G-BA assessment for services with a NUB status 1 if they involve high-risk methods.
Do I need consultation for a NUB procedure?
In principle, a consultation procedure is not necessary or possible for a NUB procedure pursuant to sec. 6 para. 2 KHEntgG.
What are the risks of a NUB process for the industry?
A distinction must first be made for the risk assessment as to whether a medical device of high-risk classes (IIb or III) is involved and whether any NUB proposals have already been submitted to the InEK in the past. Since these proposals concern technologies that are generally rated independently by manufacturers and since the proposals can also be submitted by hospitals without consulting the industry, the risk assessment is not always clear.
In addition, it must be gauged whether the procedure applied for is a new theoretical-scientific concept. The SGB V (sec.137 h) states that it is a new theoretical-scientific concept "if its principle of action or its field of application differs significantly from other systematic approaches already introduced in in-patient care".
The proposal procedure at the InEK may trigger a proposal process at the G-BA if it is the first ever NUB procedure for this method, if it is a new theoretical-scientific concept and if it is a medical device of high-risk classes IIb or III. A consultation procedure at the G-BA can be advantageous in this case.
In other cases, a G-BA advisory procedure may itself be associated with risks and, in our view, does not make sense because it may initiate an investigation at the G-BA, the result of which may be that a study must be carried out for the method. Furthermore, the InEK might not appoint it NUB status 1. We consider this constellation a high risk.
Check carefully whether you need a consultation with the G-BA. The consultation process itself may carry some risks.
What does the NUB procedure imply for the medical industry?
The NUB procedure at the InEK enables a shortcut to reimbursement in the in-patient sector for innovative medical devices.
However, it is not without risk for medical devices that are based on a new theoretical-scientific concept and are registered in class IIb or III.

What does a NUB procedure cost?
Participation in the NUB procedure in accordance with sec. 6 para. 2 KHEntgG is free for hospitals.
Costs arise only through the necessary support services.
However, these costs are overall lower than the lost opportunity costs if you do not participate in the NUB proceedings.
The right steps at the right time with experienced advisors are crucial. Get information early. "It's always too early until it's too late." (Unknown)